


Screening for advanced liver fibrosis due to MALSD alongside retina scanning in people with T2D

Study reference
Lindfors, Andrea et al. “Screening for advanced liver fibrosis due to metabolic dysfunction-associated steatotic liver disease alongside retina scanning in people with type 2 diabetes: a cross-sectional study.” The lancet. Gastroenterology & hepatology vol. 10,2 (2025): 125-137.
Background
Metabolic dysfunction-associated steatotic liver disease (MASLD) is highly prevalent in people with type 2 diabetes, with global estimates around 65% in this group.
Advanced liver fibrosis is the main predictor of morbidity and mortality in MASLD.
International guidelines recommend screening for advanced fibrosis in people with type 2 diabetes, but practical implementation strategies are lacking.
Retina scanning for diabetic retinopathy is already a routine, centralized process for people with type 2 diabetes in Sweden.
Study Objective
To assess whether vibration-controlled transient elastography (VCTE™, e.g., FibroScan®) for liver fibrosis can be efficiently and acceptably implemented alongside routine retina screening in people with type 2 diabetes, and to estimate the prevalence of MASLD and advanced fibrosis in this population.
Methods
Cross-sectional study at a large retina scanning facility in Stockholm, Sweden (Nov 2020–June 2023).
Participants were adults with type 2 diabetes referred for routine retina scanning.
Procedures
VCTE™ was performed during waiting time for retina scan.
Increased liver stiffness: ≥8.0 kPa; advanced fibrosis: >12.0 kPa.
MASLD defined as CAP™ (controlled attenuation parameter) ≥280 dB/m.
Participants with elevated or unreliable VCTE™ referred for secondary specialist evaluation.
Main Results
1005 patients (77.2%) accepted VCTE™ screening.
504/973 (51.8%) had MASLD defined by CAP™ ≥280 dB/m.
154/977 (15.8%) had liver stiffness ≥8.0 kPa (suggestive of fibrosis).
49/977 (5.0%) had liver stiffness >12.0 kPa (possible advanced fibrosis).
On repeat specialist evaluation, 56/124 (45.2%) participants with initially elevated liver stiffness had normal values (<8.0 kPa).
Final prevalence after confirmation: 74/1,005 (7.4%) had confirmed liver stiffness ≥8.0 kPa; 29/1,005 (2.9%) had >12.0 kPa.
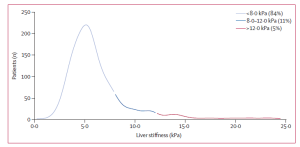
Distribution of liver stiffness by VCTE™ (kPa) from reliable measurements in 977 participants with type 2 diabetes
Prevalence Table
| Outcome | n / N | % |
| MASLD (CAP ≥280 dB/m) | 504/97 | 51.8% |
| Liver stiffness ≥8.0 kPa | 154/977 | 15.8% |
| Advanced fibrosis (>12.0 kPa, initial) | 49/977 | 5.0% |
| Confirmed liver stiffness ≥8.0 kPa | 74/1,005 | 7.4% |
| Confirmed advanced fibrosis (>12.0 kPa) | 29/1,005 | 2.9% |
Take home messages for diabetologists
- Feasibility: Screening for liver fibrosis with VCTE™ alongside retina scanning is feasible and well accepted in people with type 2 diabetes.
- High Prevalence: Over half of screened patients had MASLD; 7.4% had confirmed significant fibrosis, and 2.9% had advanced fibrosis.
- Clinical Implication: Integrating liver fibrosis screening into existing diabetes care pathways (e.g., retina clinics) can help identify patients at risk for liver-related complications, but should include a two-step VCTE™ protocol to minimize overtreatment due to false positives.
Simultaneous screening for advanced liver fibrosis using VCTE™ during routine retina scans in people with type 2 diabetes is feasible and widely accepted, enabling effective case-finding for metabolic dysfunction-associated steatotic liver disease. Authors recommend to confirm elevated VCTE™ results with a second measurement before making any clinical management decisions.